Investigators
compared cisplatin plus irinotecan to 3 other platinum-based
doublets (carboplatin plus paclitaxel, cisplatin plus gemcitabine,
and cisplatin plus vinorelbine). There was no difference in
response rates between the 4 arms. However, there are significant
differences in toxicity. Final survival data is not available
yet.
Chemotherapy provides a survival benefit
in non-small cell lung cancer. Compared with the best supportive
care, it reduces symptoms and improves quality of life. Oncologists
consider platinum-based doublets as a standard chemotherapy
for advanced non-small cell lung cancer. However, comparative
studies have not established any doublet regimen as the consistent
standard chemotherapy choice.
Investigators in a Japanese phase III trial
considered cisplatin plus irinotecan doublet to be a control
regimen. This is because cisplatin/irinotecan showed a small
survival advantage versus cisplatin/vindesine in earlier phase
III trials.
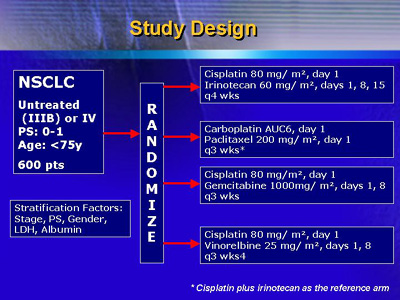
Accordingly, investigators in the Four-Arm
Cooperative Study (FACS) compared 3 platinum-based chemotherapy
doublets to a reference arm of cisplatin plus irinotecan.
The 3 comparator arms included carboplatin plus paclitaxel,
cisplatin plus gemcitabine, and cisplatin plus vinorelbine.
Investigators at 44 centers in Japan registered
600 patients (age less than 75, PS 0-1) with untreated, cytologically
documented stage IIIB/IV non-small cell lung cancer. Patient
characteristics such as age, gender and stage were well balanced
in the 4 treatment arms.
Investigators randomized the patients to following
regimens:
-
|
Cisplatin 80 mg/m2 on day 1,
irinotecan 60 mg/m2 on days 1, 8 and 15 every
4 weeks |
-
|
Carboplatin (AUC=6) on day 1,
paclitaxel 200 mg/m2 on day 1 every 3 weeks |
-
|
Cisplatin 80 mg/m2 on day 1,
gemcitabine 1000 mg/m2 on days 1 and 8 every
3 weeks |
-
|
Cisplatin 80 mg/m2 on day 1,
vinorelbine 25 mg/m2 on days 1 and 8 every
3 weeks |
Here at ASCO, Dr. Ohe reported that the objective
tumor response rate by intention-to-treat analysis was 31%
in the cisplatin/irinotecan arm. Response rates were not significantly
different for paclitaxel/carboplatin (33%), cisplatin/gemcitabine
(30%) and cisplatin/vinorelbine (33%).
Response Rates (RECIST)
Treatments
|
N
|
CR
|
PR
|
SD
|
PD
|
NE
|
Response
Rates |
P
values*
|
Cisplatin
+ Irinotecan
|
145
|
0
|
45
|
69
|
23
|
8
|
31%
|
- |
Carboplatin
+ Paclitaxel
|
145
|
1
|
47
|
58
|
34
|
5
|
33%
|
0.706
|
Cisplatin
+ Gemcitabine
|
146
|
0
|
44
|
59
|
32
|
11
|
30%
|
0.868
|
| Cisplatin
+ Vinorelbine |
145 |
0 |
48 |
57 |
31 |
9 |
33% |
0.706 |
* Compared with cisplatin plus irinotecan
using χ 2 test
|
The safety data suggest differences in toxicity
between cisplatin/irinotecan and the 3 comparator arms. For
example, frequency of grade 3-4 neutropenia was significantly
lower in the cisplatin/gemcitabine arm (61% versus 82.8%,
p < 0.05). On the other hand, cisplatin/gemcitabine had
a higher incidence of grade 3-4 thrombocytopenia (33.9% versus
6.3%, p < 0.05).
Hematological Toxicity
| |
IP
(n = 128)
|
TC
(n = 118)
|
GP
(n = 118)
|
NP
(n = 123) |
| |
Grade
|
Grade |
Grade |
Grade |
| |
|
|
|
|
Leukocytes
|
|
12 |
53 |
58 |
5 |
| (50.8%) |
(49.2%) |
|
|
21 |
43 |
49 |
5 |
| (54.2%) |
(45.8%) |
|
|
33 |
46 |
39 |
0 |
| (66.9%) |
(33.1%)* |
|
|
10 |
34 |
60 |
19 |
| (35.8%) |
(64.2%)* |
|
Neutrophils
|
|
8 |
14 |
51 |
55 |
| (17.2%) |
(82.8%) |
|
|
10 |
8 |
25 |
75 |
| (15.3%) |
(84.7%) |
|
|
20 |
26 |
49 |
23 |
| (39.0%) |
(61.0%)* |
|
|
8 |
8 |
21 |
86 |
| (13.0%) |
(87.0%) |
|
Hemoglobin
|
|
35 |
54 |
32 |
7 |
| (69.5%) |
(30.5%) |
|
|
51 |
50 |
15 |
2 |
| (85.6%) |
(14.4%) |
|
|
40 |
50 |
23 |
5 |
| (76.3%) |
(23.7%) |
|
|
33 |
54 |
30 |
6 |
| (70.7%) |
(29.3%) |
|
Platelets
|
|
|
97 |
10 |
11 |
0 |
| (90.7%) |
(9.3%) |
|
|
55 |
23 |
40 |
0 |
| (66.1%) |
(33.9%)* |
|
|
118 |
4 |
1 |
0 |
| (99.2%) |
(0.8%)* |
|
| Febrile Neutropenia |
|
108 |
- |
20 |
0 |
| (84.4%) |
(15.6%) |
|
|
99 |
- |
19 |
0 |
| (83.9%) |
(16.1%) |
|
|
116 |
- |
2 |
0 |
| (98.3%) |
(1.7%)* |
|
|
99 |
- |
24 |
0 |
| (80.5%) |
(19.5%) |
|
* Significantly
increased compared with IP (p < 0.05: using χ2 test)
* Significantly decreased compared with IP (p < 0.05:
using χ2 test)
|
At the time of this analysis, the 3 platinum-based
regimens have response rates similar to the cisplatin/irinotecan
arm. However, they have different toxicity profiles than cisplatin/irinotecan.
Dr. Ohe said investigators will conduct the final analysis
of this data in November 2003.
|