| Adding
paclitaxel to doxorubicin/cyclophosphamide had a modest benefit
in women with node-positive breast cancer. There was an improvement
in disease-free survival but not overall survival. The toxicity
of this regimen is acceptable for the adjuvant setting. The
combination may be a new alternative to the gold standard treatment.
Dr. Mamounas presented the
results of the National Surgical Adjuvant Breast and Bowel
Project (NSABP) trial B-28. This large randomized trial (n
= 3,060) tested the effect of adding Paclitaxel after Doxorubicin/Cyclophosphamide
(AC) chemotherapy in patients with node-positive breast cancer.
Investigators enrolled patients with operable breast cancer
and pathologically positive nodes. After stratification, patients
were randomized to 2 groups. The first group received standard
doses of AC (60/600 mg/m2) for 4 cycles, and the second group
received standard AC (60/600 mg/m2) followed by 4 cycles of
Paclitaxel (225mg/m2 as a three hour infusion).
Estrogen or progesterone receptor positive
patients less than 50 years of age and all patients over the
age of 50 received tamoxifen (20 mg po qd) for five years
starting with AC chemotherapy. Patients treated with lumpectomy
also received breast radiation. Patients who underwent mastectomy
did not receive radiation therapy to the chest wall or regional
nodes.
The primary endpoint of the trial was disease
free survival and overall survival. The median follow-up was
64.8 months for the AC group and 64.4 for the AC/paclitaxel
group.
The distribution of patients and tumor characteristics
was well balanced between the two arms. About half the patients
were under age 50, and about one-third were between ages 50
and 59. About two-thirds of the patients had tumors less than
2 cm in diameter; 70% of the patients had 1 to 3 positive
nodes, and only 4% had more than 10 positive nodes. Half of
the patients underwent mastectomy, and half underwent lumpectomy.
About two-thirds of the patients had tumors positive for estrogen
receptors, and also about two-thirds had tumors positive for
progesterone receptors. Eighty-four percent of the patients
received tamoxifen.
Toxicity was acceptable for the adjuvant setting,
according to Dr. Mamounas. About 27% of the patients had grade
3 or 4 toxicity during AC administration, and about 35% of
the patients had grade 3 or 4 toxicity during Paclitaxel administration.
The most common grade 3 or higher toxicities with paclitaxel
were neurosensitive toxicity in about 14%, arthralgias or
myalgias in about 11%, neuromotor toxicity in about 7%, day
1 granulocytopenia in about 4%, febrile neutropenia in 2%
and infection in 2%. Severe hypersensitivity reactions were
uncommon (1%).
There were 8 cases of acute myelogenous leukemia
or myelodysplastic syndrome, 6 in the AC followed by paclitaxel
group, and 2 in the AC group. Most of those patients had also
received prophylactic G-CSF and 5 of the 8 had also received
radiotherapy.
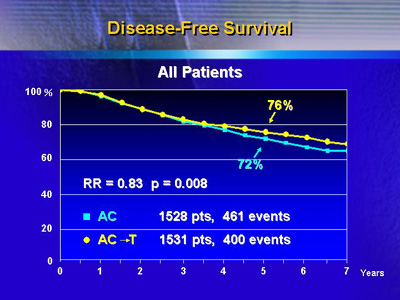
For the AC/paclitaxel group, there was a 17%
reduction in event rate for disease free survival, which was
statistically significant (p = 0.008). The actual events were
461 in the AC group and 400 in the AC/Paclitaxel group. There
was no statistically significant difference in survival, with
deaths being 255 in the AC group and 243 in the AC/Paclitaxel
group.
|
Disease-Free Survival and
Survival
All Patients
| |
AC
1528 pts |
AC→T
1531 pts
|
RR*
(95%CI) |
p
value |
| Events |
461 |
400 |
0.83
(0.73-0.95) |
0.008 |
| Deaths |
255 |
243 |
0.94
(0.78-1.12)
|
0.46 |
* RR Adjusted for # (+) nodes, operation,
TAM use
|
Five-year disease-free survival was 72% for
AC, and 76% for AC/Paclitaxel. Overall survival was the same
(85%) for both groups.
Looking at the incidence of first events at
specific sites, there was evidence of a reduction in all subsets,
including local recurrence, regional recurrence, distant recurrence,
other second primary cancers, or death with no evidence of
disease.
|
5-Year Cumulative Incidence
of
First Events at Specific Sites
| |
AC
1528 pts(%) |
AC→T
1531 pts(%)
|
Local Reccurrence
Regional Reccurrence
Distant Reccurrence
Opposite Breast
Other Second Primary Cancer
Dead with No Evidence of Disease
|
4.7
2.9
14.9
1.6
2.9
1.1 |
4.2
2.2
13.9
0.9
2.1
1.0 |
| All 1st Events |
28.1 |
24.4 |
|
There was also a subset analysis looking at
the effect of Paclitaxel according to hormone receptors. Prior
study results suggest that paclitaxel is not very effective
in receptor-positive patients. The disease free survival according
to hormone receptor status showed that there was a 21% reduction
in events rate in hormone receptor positive patients versus
a 9% reduction in hormone receptor negative patients; however,
this difference did not reach statistical significance.
Dr. Mamounas said there are now 3 studies
showing that taxanes are beneficial in women with node-positive
breast cancer. NSABP B-28 is the second study that shows a
benefit with the addition of paclitaxel to the standard regimen
of AC (the first study was CALGB 9344). In addition, investigators
have reported results of a similar study of docetaxel following
AC chemotherapy; that study also showed a benefit in disease-free
survival and a non-significant benefit in overall survival.
Taken together, these results suggest
there is now another option for patients with node-positive
breast cancer that can actually improve their survival above
and beyond the administration of anthracyclines, which have
been the gold standard for many years.
|