Lymphatic Mapping and Sentinel Lymphadenectomy: A Novel Technique to Improve Staging in Patients with Gastrointestinal Neoplasms.
Anton J. Bilchik, M.D., PhD, John Wayne Cancer Institute, Santa Monica, CA, USA
Summary: Lymph node analysis is essential for staging gastrointestinal neoplasms. Intraoperative lymphatic mapping and sentinel lymphadenectomy are now under investigation to improve staging of gastrointestinal neoplasms. Focused analysis of the sentinel node seems to be highly sensitive for detection of micrometastases; thus, it may improve selection of patients for adjuvant treatment.
Lymphatic mapping and sentinel node dissection differ for gastrointestinal tumors compared with melanoma and beast cancer. In those cancers, sentinel node tracing and dissection minimize unneeded adjuvant surgery and morbidity. With gastrointestinal tumors, the technique primarily allows pathologists to locate the sentinel node more carefully.
Isosulfan blue dye is injected into the periphery of the gastrointestinal tumor. Lymphatic flow is traced to the sentinel node, which is marked with a suture. The tumor, the sentinel node, and all other nodes in the same region are removed en bloc. In a study of 126 patients, Dr. Bilchik found an average of 1.7 sentinel nodes (range 0-4) and an average total of 15 lymph nodes per patient. Samples from each node were analyzed with multiple sectioning, hematoxylin and eosin staining, and cytokeratin immmunohistochemistry.
In 20% of patients who were sentinel node-negative by hematoxylin and eosin staining, testing was positive after the additional steps of multiple sectioning and cytokeratin immunohistochemistry. This resulted in upstaging of patients with large and small bowel cancer (18% and 25% respectively), stomach cancer (30%), and pancreatic cancer (25%).
Dr. Bilchik found that micrometastases were inversely proportional to tumor size. "The smaller the tumor, the greater the chance the sentinel node contained micrometastases found by cytokeratin immunohistochemistry," he said. "This made us think about how we do surgery."
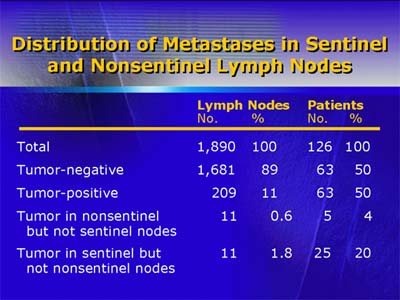
He cautioned about the complexities of using sentinel node mapping for patients with gastrointestinal tumors, noting one case in which a cancer of the right colon had metastasized to a lymph node on the left side. Such atypical lymphatic drainage was found in 8% of cases and expanded the extent of subsequent lymphadenectomy. In addition, there is the possibility of a false negative when the involved sentinel node is obliterated by the tumor itself and lymphatic flow cannot be traced. Conventional pathologic dissection may then be needed to identify and remove the involved nodes.
A variant approach uses endoscopically injected technetium and lymphoscintigraphy. If the sentinel node is negative, minimal surgery is used to remove the tumor and the sentinel node. This technique may change management of gastric cancer in early-stage patients, enabling surgeons to avoid radical surgery and its associated morbidity.
In conclusion, Dr. Bilchik said that lymphatic mapping and sentinel node dissection improves selection for adjuvant treatment, although he offered no data about its prognostic value.