|


|
Summary:
In clinical trials, major advances have been made in replacement within
cancer cells of missing or non-functional tumor-suppressor genes.
Clinical trials using this strategy have focused on replacing the
tumor-suppressor gene p53. The majority of patients in these trials
have demonstrated incorporation of the virus-delivered p53 gene in
tumor cells with associated increases in apoptosis of malignant cells.
Multiple strategies use gene therapy to attack cancer cells. Dr. Jack Roth highlighted some of the most promising approaches that have reached clinical trials. Major advances have been made in replacement of missing or non-functional tumor-suppressor genes in cancer cells. Dr. Roth noted that although several mutations are necessary to achieve transformation in cancer cells, early studies have demonstrated that correcting only one of the defective genes (to produce a functionally normal allele) may be sufficient to halt tumor progression. 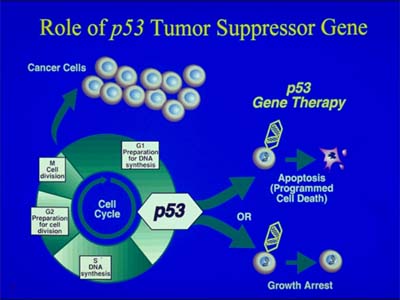
Clinical trials using this strategy have focused on replacing the tumor-suppressor gene p53. More than 50% of all types of cancer cells show mutations in the p53 gene. Altered p53 is associated with poor prognosis in many cancer patients. Tumor regression after p53 gene replacement is thought to occur by restoration of apoptosis (programmed cell death). 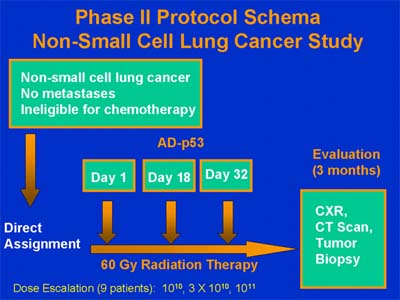
Although earlier trials used retroviral vectors, adenoviruses have proven more efficient for gene delivery. In trials using this approach, p53-containing viruses were injected directly into a patient's tumor. The majority of patients have demonstrated incorporation of the virus-delivered p53 gene into tumor cells with associated increases in apoptosis. In one example of a Phase I trial of patients with non-small cell lung cancer treated with cisplatin and adenovirus-delivered p53, 79% of tumor biopsies were found to have increased apoptosis. Notably, 75% of the patients in this trial had experienced tumor progression when treated with cisplatin alone. 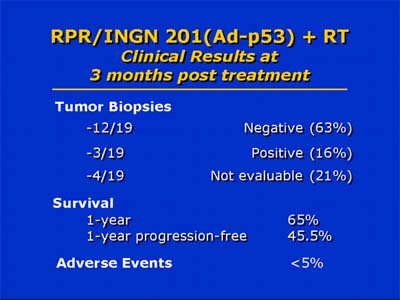
In a Phase II trial of non-small cell lung cancer patients who received p53 along with radiation therapy, complete or partial responses were achieved in 44% of patients and one-year progression-free survival was 45%. This is a notable improvement over the three-month pathologic control rate of 17% reported for radiation treatment alone. 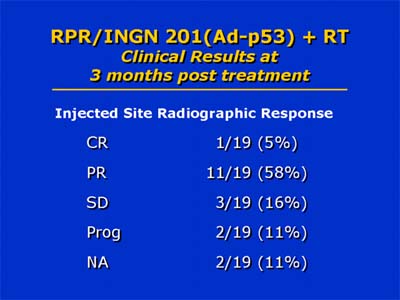
Other gene therapy approaches to cancer treatment have included insertion of genes into cancer cells to sensitize them to chemotherapy. The first clinical trial to use this strategy involved transfection of brain tumor cells with the herpes simplex virus thymidine kinase gene. Subsequent treatment with gancyclovir resulted in production of cytotoxic gancyclovir triphosphates in these cells. Overall, Dr. Roth noted that contrary to initial predictions, virus-assisted gene transfer has been more efficient in cancer cells than in normal tissue cells, with viral vectors spreading readily throughout a solid tumor. Few complications have arisen from gene-transfer, which has enabled some patients to undergo treatment on an outpatient basis. Results of gene therapy in combination with other treatment modalities have been particularly encouraging. |
| Reporter: Jill Waalen, M.D. |