| Diabetics with
heart failure symptoms who received a beta-blocker did not have an
excess risk of hyperglycemia or renal dysfunction. All-cause mortality
was not different between diabetics and non-diabetics. These results
suggest physicians should not withhold beta-blockers from diabetics.
Beta-blockers have established value in treating heart failure.
However, many physicians are hesitant to use beta-blockers in heart
failure patients who have diabetes. This is mainly because they
fear beta-blockers may exacerbate glucose intolerance.
About one-third of heart failure patients have diabetes mellitus.
Dr. Fowler and colleagues wanted to know if there is evidence to
justify concerns over using beta-blockers in these patients. They
examined the effect of carvedilol versus placebo in patients who
participated in the COPERNICUS trial.
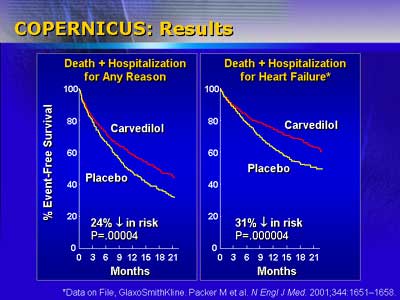
Investigators in this trial randomized 2,289 patients with heart
failure symptoms at rest or on minimal exertion to carvedilol or
placebo. They stopped the trial early because carvedilol markedly
improved survival.
That patient population included 589 diabetic and 1,700 non-diabetic
patients. Dr. Fowler reported that both diabetic and non-diabetic
patient groups had a similar improvement in clinical status, rate
of hospitalization and survival.
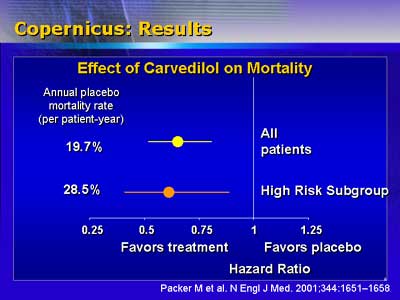
Hazard ratios (treatment/placebo) for all-cause mortality were
0.65 for both diabetics and non-diabetics. Hazard ratios were also
similar for composites of all-cause mortality and hospitalization.
Diabetics tolerated carvedilol well, according to Dr. Fowler. They
had no excess risk of hyperglycemia or renal dysfunction. There
was a low incidence of hypotension and presyncope in these patients.
Dr. Fowler said physicians should not fear that carvedilol treatment
would harm diabetics. In fact, this treatment effectively reduces
death and hospitalization in these patients.
|

