| The current mindset
for treatment of mitral regurgitation should be to "do something
now." That is unlike the conventional thinking, which has been
to wait until the prognosis is dire before electing surgical intervention.
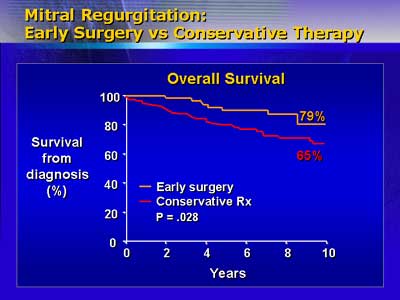
The rationale for this change lies in poor outcomes with conservative
medical management, and advances in surgical technique.
About 39 % of mitral regurgitation patients with left ventricular
ejection fractions <60% are dead within 10 years of diagnosis.
Their annual death rate is 1.8%. The sudden death rate for patients
with ejection fractions <50% is 13%. The ejection fraction predicts
post-operative survival. While survival is extremely poor with ejection
fractions <50% and better with ejection fractions >60%, excess
mortality is evident between 50-60%. Post-operative left ventricular
dysfunction, also increases markedly as end systolic diameters go
beyond >45 mm. Dr. Sarano said that the conservative thinking
that views >60% ejection fraction and <45 mm diameter as acceptable
for medical management is not really valid, because most who die
of sudden death are asymptomatic and have good left ventricular
function. Also, experience at the Mayo Clinic with 600 mitral regurgitation
patients is that left ventricular dysfunction starts much earlier.
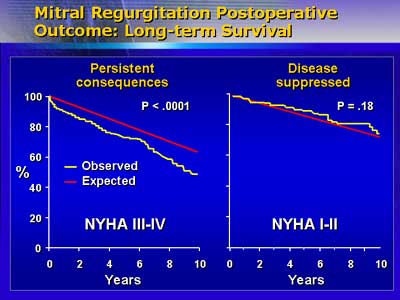
The difficulty is that physicians are fooled by the apparent improvements
brought by medical therapy. But waiting for class III-IV symptoms
to appear entails a 5% operative mortality risk-as compared with
the 10-fold higher 5% risk among patients with minimal or no symptoms.
Also, the long-term postoperative mortality for those with severe
pre-operative symptoms is much higher than for class I or II symptoms.
Mitral regurgitation is a progressive disease, as shown via echocardiography
by 7-8 ml increases in regurgitation volume per year. Within 15
years, 97% of patients in class I or II will require surgery and
58% will develop heart failure. Surgical treatment for these patients,
however, brings their mortality risk into expected range.
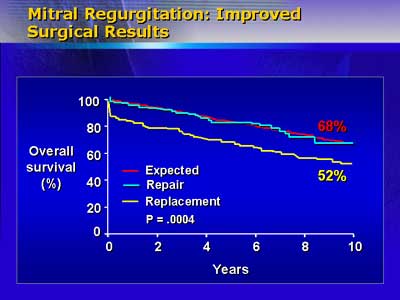
Also contrary to conventional wisdom, mitral valve repair is preferable
to valve replacement, with better long-term survival for repair
of both anterior and posterior leaflet prolapse as compared with
replacement. Technical improvements in the last decade have markedly
reduced need for re-operation, and support an early surgical strategy.
Dr. Sarano concluded that when valves are reparable, ejection fraction
is >60% and patients are in class I or II, such an approach offers
the best outcomes. The new mindset is to quantify mitral regurgitation
and think "intervention now."
|

