|
Dr. Zoghbi noted echocardiography
is valuable when the admission differential diagnosis includes aortic
dissection or pericarditis. After admission, echocardiography may
be used to diagnose complications. Most of the presentation, however,
focused on echocardiography in the setting of pre-discharge risk
stratification. In this context, Dr. Zoghbi mentioned at rest and
stress testing, especially with use of dobutamine.
Dr. Zoghbi opened by noting that echocardiography
can be important before admission when the electrocardiogram is
not definitive and the differential diagnosis includes aortic dissection
or pericarditis. After admission to a coronary care unit, echocardiography
may be useful in the diagnosis of mechanical or hemodynamic complications
such as mitral regurgitation or effusion with tamponade.
Most of the presentation focused on the role of echocardiography
in pre-discharge risk stratification of patients who have had an
uncomplicated infarction. Dr. Zoghbi noted that physicians who want
to do an evaluation at rest and with stress can now obtain both
with echocardiographic assessment.
Testing at rest provides information on several prognostic factors:
ejection fraction, degree of left ventricular remodeling (with increased
end systolic volume or end diastolic volume), and mitral flow velocity
(with increased filling pressure by Doppler). Testing at rest also
allows physicians to check for multiple vessel disease and signs
of residual ischemia.
Stress testing with dobutamine infusion allows the physician to
evaluate contractile reserve (at lower doses) and residual viability
and ischemia (at near maximal doses).
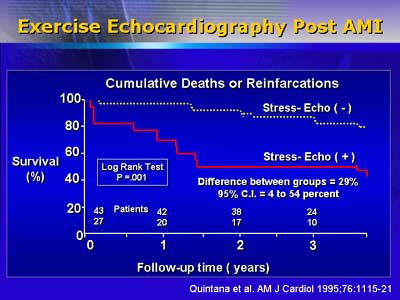
In an Italian series of over 8000 patients (Nicolosi, 1996), echocardiography
at a mean time of 12 days post-infarction was found to be safe and
was predictive for unstable angina, recurrent infarction, or death.
Evaluation was primarily done with high-dose dobutamine evaluating
for wall motion abnormalities indicative of ischemia.
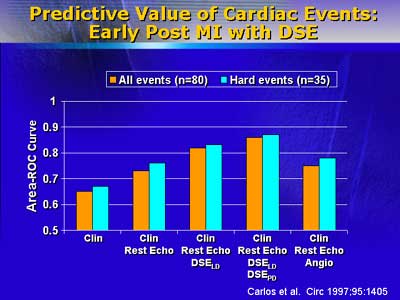
A study by Carlos and colleagues with roughly 200 patients demonstrated
that the predictive power of resting/stress echocardiography (the
latter with low-dose and high-dose dobutamine infusion) was superior
to that of the combination of electrocardiogram, clinical data,
and resting ventricular function.
Dr. Zoghbi also mentioned that the value of echocardiography may
vary depending on the primary therapy for the infarction itself.
He stated that the value of the imaging technique for patients who
have had thrombolytic therapy is generally very high. It is generally
lower for patients who have had angioplasty except in cases where
the physician is looking for additional coronary artery disease.
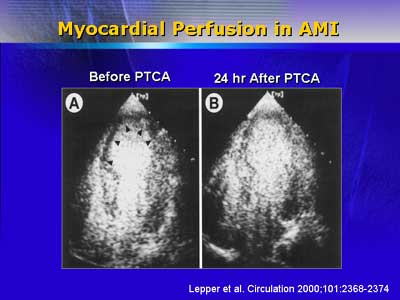
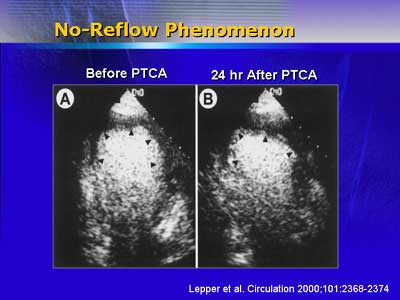
He concluded by mentioning that the future of contrast echocardiography
is promising and includes roles in assessment of left ventricular
function and myocardial perfusion.
|

