| Non-pharmacologic
therapies currently used to treat atrial fibrillation are grouped
into those that control rate, those that maintain sinus rhythm, and
those that ablate the initiators. Heart rate is controlled by AV node
ablation with pacemaker or AV node modification without pacemaker.
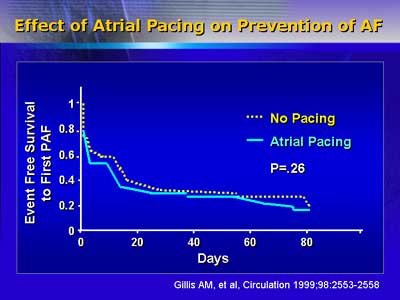
Sinus rhythm is maintained with adjunctive pacing, implantable atrial
defibrillator, surgical maze procedures and catheter ablation.
Non-pharmacologic therapies currently used to treat atrial fibrillation
are categorized into those that control rate, those that maintain
sinus rhythm and those that ablate the initiators of atrial fibrillation.
Heart rate can be controlled by two methods, AV node ablation with
pacemaker or AV node modification without pacemaker. Sinus rhythm
can be maintained with adjunctive pacing, implantable atrial defibrillator,
surgical maze procedures and catheter ablation.
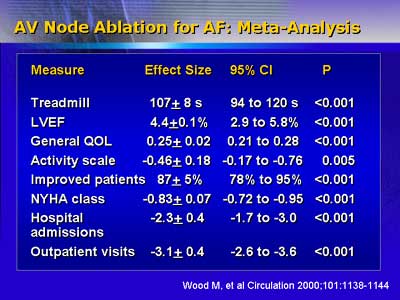
AV node ablation generates a complete heart block and requires
a permanent pacemaker to control heart rate after the procedure.
This technique controls symptoms, improves quality of life, decreases
the use of anti-arrhythmic medications, reduces hospital admissions
and outpatient visits. AV node modification slows AV node conduction
just before a complete heart block. For this reason, a permanent
pacemaker is not needed. The procedure has the risk of complete
heart block because the endpoint is difficult to assess. Studies
that compared these two techniques demonstrated more symptom control
and fewer hospital visits with AV node ablation. These approaches
are indicated for patients whose ventricular rate does not respond
to medical therapy; who cannot tolerate medical therapy; whose atrial
fibrillation causes exacerbations in heart failure, angina, hypertension
or precipitated ventricular fibrillation; and whose treatment of
co-morbid illness prevents regulation of atrial fibrillation.
Maintenance of sinus rhythm is best achieved with implantable atrial
defibrillators or surgical maze procedures. Implantable atrial defibrillators
contain atrial pacing and rate stabilization algorithms and tiered
atrial fibrillation therapy built into them. Their use is limited
to patients with infrequent episodes of atrial fibrillation and
ventricular tachyarrhythmias. Surgical maze procedures limit the
capability of the atria to maintain atrial fibrillation once initiated.
The most successful and curative procedure is isolation of the pulmonary
vein to the mitral annulus. More studies are needed to determine
the clinical role of adjunctive pacing and catheter ablation.
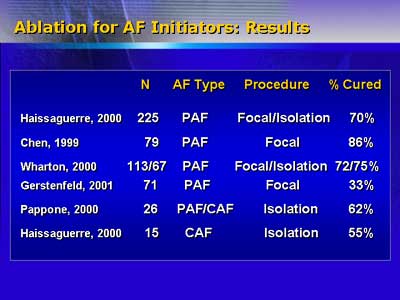
Because most initiation sites for atrial fibrillation occur within
the pulmonary vein, the pulmonary vein isolation procedure has a
success rate of 90% of cure or palliation. This procedure prevents
conduction into or out of the vein. The best candidates for this
procedure are patients with paroxysmal or persistent atrial fibrillation
who are symptomatic and refractory to drugs and have minimal to
moderate structural disease. Dr. Wharton believes ablation therapy
will be used to cure more cases of atrial fibrillation in the future.
|

