CAPRICORN:
A Multinational, Randomized, Double-Blind Study of the Effects
of Carvedilol on Mortality and Morbidity in Patients with Left
Ventricular Dysfunction after Myocardial Infarction
Henry
J. Dargie
University of Glasgow Royal Infirmary, Glasgow,
Scotland, UK
Previous
studies investigating the value of beta-blocker therapy in patients
with acute myocardial infarction were done many years ago, before
the availability of therapies with thrombolysis and ACE inhibitors
and before the widespread use of aspirin. The CAPRICORN trial
results show that long-term use of carvedilol in patients treated
following acute myocardial infarction with left ventricular
dysfunction substantially reduced the incidence of all-cause
and cardiovascular mortality and of recurrent non-fatal myocardial
infarctions.
The CAPRICORN trial is the first large-scale, placebo-controlled
trial of beta-blocker therapy for patients with acute myocardial
infarction to be done in the modern era, with its widespread
use of aspirin and availability of thrombolysis and angiotensin-converting
enzyme (ACE) inhibitors. In addition, many of the earlier trials
excluded patients with heart failure. CAPRICORN studied the
use of carvedilol among patients who had acute myocardial infarction
with left ventricular dysfunction -- that is, patients who had
a decreased ejection fraction (<40%) with or without clinical
heart failure. The study included 1,959 patients randomized
to receive a placebo or carvedilol at doses titrated up to 25
mg twice daily. (Dr. Dargie noted that 75% of patients in the
active treatment group received the maximum dose and tolerated
it well.) Treatment was initiated within 3 to 21 days after
the acute event; the average time for initiation of treatment
was approximately 10 days. Patients were followed for a mean
of 1.3 years.
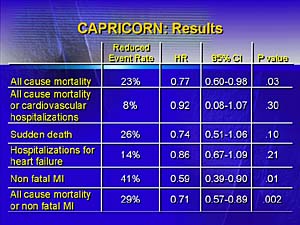
Dr. Dargie said that the data show carvedilol reduced all-cause
mortality by 23% (p = .03), non-fatal myocardial infarctions
by 41% (p = .01), and all-cause mortality or non-fatal myocardial
infarction by 29% (p = .002). There was a trend toward decreased
hospitalizations in the carvedilol group, but it was not statistically
significant. Dr. Dargie said: "Please note that the number
of patients we need to treat with carvedilol for 1 year to prevent
1 death is 43, which is a very favorable number and is comparable
to the number for ACE inhibitors. However, this effect with
carvedilol is additive to the effect of ACE inhibitors, so if
patients receive both drugs they will receive the combined beneficial
effects."
Dr. Dargie concluded: "The results of the CAPRICORN trial
bridge the gap between treatment of patients in the Cardiac
Care Unit and the treatment of congestive heart failure. Since
the Cardiac Care Unit is in many cases the 'birthplace' of cases
of congestive heart failure, we may expect carvedilol therapy
in patients with acute myocardial infarction with left ventricular
dysfunction to reduce the number of patients in this situation
who progress to overt heart failure."
Reporter:
Andre Weinberger, MD
Copyright
2000-2013 by HESCO International, Ltd. All rights reserved.