The
Aggressive Diagnosis of Restenosis (ADORE) Trial
Mark
J. Eisenberg
McGill University, Montreal, Quebec, Canada
Patients
who undergo percutaneous coronary intervention (PCI) are at
risk for restenosis of the previously occluded vessel. The results
of this study clearly demonstrate that routine diagnostic monitoring
for evidence of restenosis after PCI does not confer any clinical
benefit compared with testing patients only if and when symptoms
of ischemia develop.
Dr. Eisenberg began by observing there are more than 700,000
percutaneous coronary intervention (PCI) procedures done every
year in North America and more than 175,000 cases of restenosis
following PCI. There is no substantial consensus among cardiologists
regarding follow-up for patients after PCI: Should routine testing
for evidence of restenosis be done, or should patients be tested
only if and when symptoms of ischemia develop to suggest the
possibility of reocclusion? There are very few data in the medical
literature to guide us in resolving this question. "We
saw a need for reliable clinical data to help us deal with this
common and important question, and we designed and executed
this clinical trial in an attempt to provide such data."
In this study, 348 patients who underwent PCI were enrolled.
Of that total, 172 were randomized to the routine diagnostic
study group and 176 to the "selective" or "clinically
driven" strategy. Patients were followed for 9 months,
and those in the routine diagnostic studies group underwent
exercise testing 6 weeks after PCI and exercise testing plus
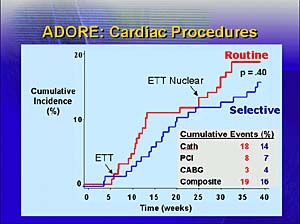
a nuclear cardiography scan 6 months after PCI. The results
were surprising: The routine studies group accounted for 94%
of all diagnostic testing done -- fifteen times more than the
number of tests done for the clinically driven studies group.
Interestingly, although there were many positive tests in the
routine studies group (more than 30%), the rates of cardiac
procedures done were similar in the two groups. Dr. Eisenberg
explained: "We were concerned that a high rate of positive
tests in a group undergoing frequent diagnostic studies would
translate into a large number of repeat revascularization procedures.
However, not all positive results are the same, and apparently
the cardiologists were acting appropriately in deciding which
positive tests served as indications for a revascularization
procedure, and which did not."
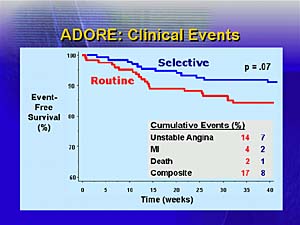
In general, the two approaches were
similar in all measured outcomes. Several questionnaires were
used to evaluate health-related Quality of Life, and results
of these measures were similar for both groups. In terms of
survival, the two groups were similar, with a trend toward poorer
survival in the routine studies group. Dr. Eisenberg concluded:
"Overall, there is no greater clinical benefit associated
with routine testing for evidence of restenosis after PCI compared
with symptom-based testing. This study was not sufficiently
powerful to distinguish between higher-risk and lower-risk patients,
but we are looking into that issue in an ongoing study."
Reporter:
Andre Weinberger, MD
Copyright
2000-2013 by HESCO International, Ltd. All rights reserved.