Management
of the Hemodynamically Compromised Patient with Acute MI
Kanu
Chatterjee
University of California,
San Francisco, California, USA
Physicians
naturally focus immediate attention toward correcting hemodynamic
abnormalities in hemodynamically compromised patients. However,
in patients presenting with acute myocardial infarction and
hemodynamic compromise, the first step should be early and adequate
reperfusion.
Patients with acute myocardial infarction (MI) often present
with impaired hemodynamic function. Dr. Chatterjee acknowledged
that it is natural for physicians treating such patients to
focus on correcting the hemodynamic abnormalities with measures
such as inotropic support and fluids. However, he insisted that
the first step with such patients should be immediate and adequate
reperfusion therapy. He supported this recommendation by citing
data from the SHOCK trial, a 30-day survival study indicating
that immediate reperfusion in these patients is essential and
is associated with increased survival.
Dr. Chatterjee
then reviewed several clinical causes of hemodynamic compromise
in patients with acute MI. After briefly mentioning the very
common cause of left ventricular systolic or diastolic dysfunction,
he spent most of his time talking about less common causes
(two examples of which are inappropriate autonomic response
and right ventricular infarction).
Inappropriate autonomic response is characterized by three
signs: (1) hypotension, (2) an inadequate increase in systemic
vascular resistance and heart rate, and (3) normal or low
cardiac output. Treatment includes atropine and atrial pacing.
In hypovolemic shock, both right and left ventricular preloads
are decreased. Treatment involves volume expansion and monitoring
the patient for changes in right atrial pressure and pulmonary
capillary wedge pressure.
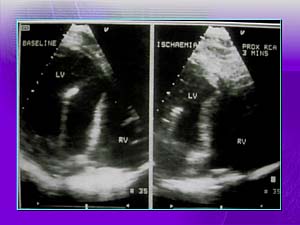
Another subset of patients presenting with hemodynamic compromise
is made up of individuals with right ventricular infarction.
In these patients, hemodynamic parameters are affected by
pericardial constrictive pressure and decreased left ventricular
preload. There may also be impairment of left ventricular
contractile function, although the mechanism for this is not
known. These patients should not receive major volume loading
because that will worsen diastolic function; inotropic agents
may be effective. Treatment should include (1) adequate reperfusion,
(2) inotropic drugs, and (3) atrial-ventricular sequential
pacing in patients with atrioventricular block. Volume loading
may be appropriate in some patients with very low right atrial
pressures.
Reporter:
Andre Weinberger, MD
Copyright
2000-2013 by HESCO International, Ltd. All rights reserved..