|
Antidepressants often induce mania and
rapid cycling in bipolar patients. Guidelines for the treatment
of bipolar patients include the preferred use of multiple mood
stabilizers. Suicidal patients are always treated with antidepressants.
Selective serotonin reuptake inhibitors (SSRIs) are the drugs
of choice. After 2 months of euthymia, patients are tapered
off the antidepressant. Patients who fail two tapering regimens
are maintained on antidepressants. Algorithms to guide the long-term
treatment of bipolar disorder are provided.
Bipolar depression is often treated with standard mood stabilizers
and antidepressant medications. Antidepressants are known
to worsen the course of bipolar illness by inducing mania
or rapid cycling. It is estimated that 25 to 50% of bipolar
patients with rapid cycling started cycling as a result of
antidepressant medications. For this reason, the clinical
value of adding antidepressants to monotherapy with lithium,
divalproex, or lamotrigine is unclear.
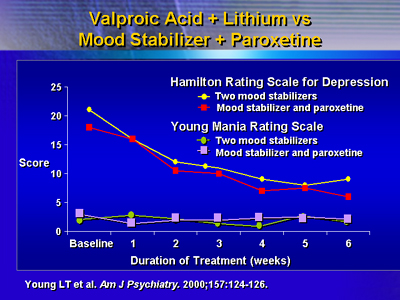
Dr. Ghaemi compared data from a recent study that treated
bipolar patients with mood stabilizers alone and mood stabilizers
combined with antidepressants. In a 6-week double-blind study,
patients were divided into two groups.One group received valproate
plus lithium. The other group was treated with mood stabilizer
and paroxetine.Both groups were evaluated for bipolar symptoms
using the Young Mania Rating Scale and the Hamilton Rating
Scale for Depression.
The results indicate that both groups responded in a similar
manner. From this data, Dr. Ghaemi concluded patients do not
respond better to antidepressants. Dr. Ghaemi prefers to treat
bipolar patients with multiple mood stabilizers. However,
suicidal patients are always treated with antidepressants.
Antidepressants are chosen based on lowest likelihood of inducing
mood switching to mania. Dr. Ghaemi prefers to treat patients
with selective serotonin reuptake inhibitors (SSRIs) rather
than tricyclic antidepressants (TCAs). In particular, paroxetine,
bupropion and citalopram are used before other antidepressants.
After 2 months of euthymia, patients are slowly tapered off
the antidepressant. Patients who fail two tapering regimens
are maintained on antidepressants. Dr. Ghaemi estimates his
use of antidepressants in bipolar patients is 20 to 50%.
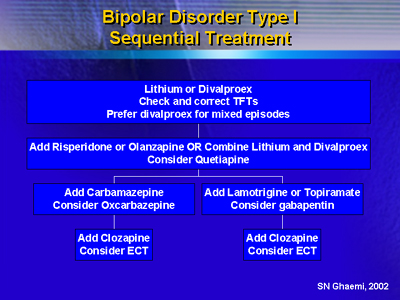
Dr. Ghaemi presented this information in two algorithms.One
algorithm was designed to aid clinicians in the long-term
treatment of bipolar I patients.
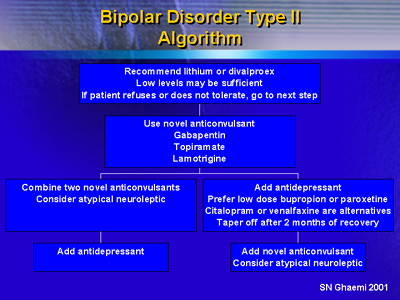
The second algorithm provides guidelines for the long-term
treatment of patients with bipolar II disorder.
|