|
The long-term outcome of schizophrenia
is determined by a number of factors that include gender, age
of onset, duration of untreated illness and associated comorbid
disorders. Dr. Schooler noted the importance of diagnosing comorbid
psychiatric conditions and syndromes such as anxiety disorders,
depression, substance and alcohol use. The impact of these comorbid
conditions on treatment was discussed.
The long-term outcome of schizophrenia is determined by
a number of factors that include gender, age of onset, duration
of untreated illness and associated comorbid disorders. Regarding
gender, the long-term outcome is better for women than for
men. The reason for this gender response is unknown. Patients
who present later in life have a better long-term course.
Patients who present early in life and have cognitive and
intellectual impairments have poorer prognoses.
Dr. Schooler noted the importance of diagnosing comorbid
psychiatric conditions and syndromes. Comorbid conditions
commonly associated with schizophrenia are anxiety disorders,
depression, substance and alcohol use. Comorbid conditions
such as these can negatively affect treatment as well as outcome.
Dr. Schooler believes the DSM-IV decision tree for schizophrenia
is the main reason comorbid conditions are often missed. She
explained that this decision-tree directs clinicians to psychotic
disorders instead of anxiety or other disorders. Physicians
should be aware of this fact when diagnosing comorbid disorders
in schizophrenic patients.
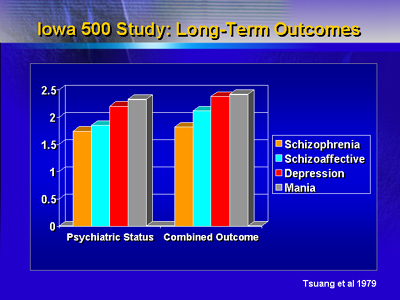
Dr. Schooler noted that information on long-term follow-up
for schizophrenic patients with comorbid conditions is limited.
In fact, many studies exclude patients with comorbid conditions.
Dr. Schooler presented data from a long-term (30 to 40 year)
outcome study that was conducted at the Iowa State Hospital.
Patients were divided into groups according to their medical
records on admission to the hospital. The results indicate
that schizophrenic patients had the poorest outcome. Schizophrenic
patients fared worse than patients with mania, depression
and schizoaffective disorders.
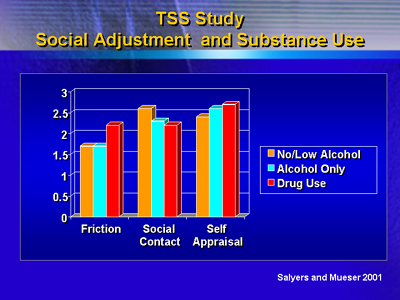
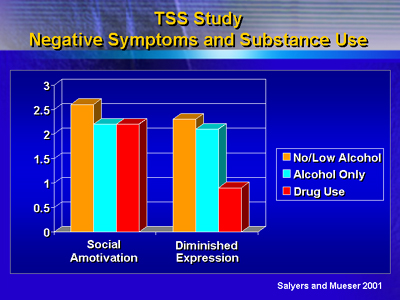
Dr. Schooler emphasized the importance of the comorbid conditions
of substance and alcohol abuse and dependence in schizophrenic
patients. Statistically, 25 to 35% of schizophrenics have
comorbid substance abuse and dependence problems. Over the
course of a lifetime, these comorbid conditions are manifested
by 50% of schizophrenic patients. Dr. Schooler showed data
from the Treatment Strategies in Schizophrenia (TSS) study
which compared treatments and psychosocial approaches in schizophrenic
patients with and without comorbid substance and alcohol use.
The results indicate substance use allows patients to function
better in social situations.
Schizophrenic patients with these comorbid conditions felt
less satisfied with their lives than schizophrenic patients
without these comorbid problems.
Schizophrenic patients with comorbid conditions can receive
treatment for their comorbid conditions. The clinician should
be aware that the comorbid conditions may alter the patient's
response to antipsychotic agents. In addition, psychosocial
approaches may be different for patients with and without
comorbid conditions. Dr. Schooler recommends that clinicians
listen to patients and ask questions in a non-threatening
way in order to develop a good rapport and relationship with
their schizophrenic patients.
|