|
Patients with schizophrenia are 5 to
6 times more likely to have a problem with violent behavior
than people without any diagnosed mental disorder. Comorbid
substance abuse increases the probability of violent behavior
further. Treatment with atypical antipsychotics, mood stabilizers,
beta-blockers and serotonin-specific reuptake inhibitors were
discussed.
Violence is pervasive in our culture. Some, but not all,
people with mental illness have problems with violence. About
50% of patients with schizophrenia exhibit violent behavior.
These patients are 5 to 6 times more likely to have a problem
with violent behavior than people without any diagnosed mental
disorder. Comorbid substance abuse increases the probability
of violent behavior further. Patients that exhibit violent
or threatening behavior are often admitted to a psychiatric
inpatient facility. Upon admission, these patients should
be assessed for the possibility of comorbid conditions.
Treatment approaches depend on the underlying clinical problem.
Short-term sedation with lorazepam is a safe and effective
choice for acute agitation. However, sedation is not an acceptable
method of treatment. Preferred treatments for acute agitation
are intramuscular preparations of the atypical antipsychotics
such as clozapine, olanzapine and quetiapine. Longer-term
solutions include strategies that treat impulsivity. Mood
stabilizers, such as valproate, carbamazepine and lithium
may be used. Valproate is often used with neuroleptics to
decrease the intensity and frequency of agitation and poor
impulse control. Beta-blockers such as propranolol and nadolol
may be used as an adjunctive agent to antipsychotics for aggression
and schizophrenia. The anti-aggressive effect of beta-blockers
may be delayed by 4 to 6 weeks. Benzodiazepines such as clonazepam
are not effective in this population and may worsen aggressive
behavior. Recent research has shown the serotinergic neurotransmitter
system may be involved in aggressive behavior. For this reason,
adjunctive serotonin-specific reuptake inhibitors (SSRIs)
may be used to treat this population. These drugs include
fluoxetine and citalopram.
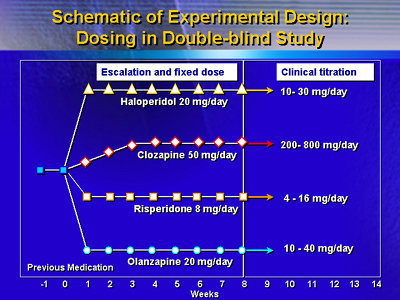
Dr. Citrome showed data from a double-blind study that treated
157 patients with either haloperidol, clozapine, risperidone
or olanzepine for 14 weeks. The experimental design is shown
below:
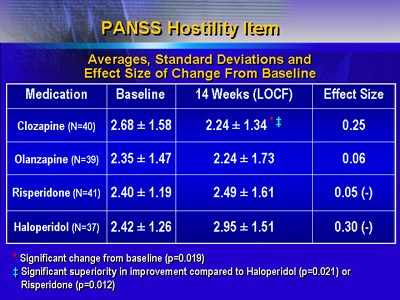
The primary outcome measure was the PANSS hostility item.
On this scale, the number 1 represents no hostility while
the number 7 indicates extreme hostility. The data indicate
clozapine significantly reduced hostility in these patients.
In contrast, risperidone and haloperidol did not affect hostility.
From these results, Dr. Citrome concluded that clozapine
was more effective than typical antipsychotics in decreasing
aggressivity in schizophrenia and superior to risperidone
and haloperidol in reducing aggressivity in patients with
schizophrenia or schizoaffective disorder.
|