|
Carvedilol may reduce plasma renin and
aldosterone levels in patients with heart failure and left ventricular
systolic dysfunction who take an angiotensin converting enzyme
inhibitor (ACE inhibitor). This finding may help explain the
apparently more-than-additive benefit of carvedilol combined
with an ACE inhibitor in patients with heart failure.
Beta-blockers in combination with ACE inhibitors are effective
treating heart failure in patients with left ventricular systolic
dysfunction. However, the mechanism of action is unclear.
To evaluate the biochemical role of beta-blockers in heart
failure patients with left ventricular systolic dysfunction,
investigators measured plasma renin activity and aldosterone
concentrations among patients in an international, double
blind, multicenter, randomized, parallel group trial. Investigators
called this study Carvedilol Hibernation Reversible ISchaemia
Trial: MArker of Success (CHRISTMAS).
The CHRISTMAS study included heart failure patients with
left ventricular systolic dysfunction due to ischaemic heart
disease and chronic stable heart failure (NYHA Class I, II,
or III). About 60% of the patients had hibernating myocardium,
regions of myocardium with reduced coronary perfusion that
caused persistent left ventricular dysfunction. The main purpose
of the study was to determine if presence of hibernating myocardium
predicted degree of improvement in left ventricular ejection
fraction.
All patients in CHRISTMAS received standard medications,
including an ACE inhibitor, if they could tolerate them. Investigators
randomized the patients to receive placebo or carvedilol for
6 months. There was a 2-month up-titration phase to the highest
tolerated dose (6.25, 12.5, 25, or 50 mg bid), and an additional
4-month maintenance phase.
The intent-to-treat analysis included 305 patients (142
on carvedilol, 163 on placebo). The mean age was approximately
62 years and the mean ejection fraction at baseline was approximately
30%. ACE inhibitors were used by 87% of patients.
Investigators previously presented the main results of CHRISTMAS.
For all patients, mean left ventricular ejection fraction
rose on carvedilol compared with placebo (increase of 2.8%
vs. decrease of 0.4%; p=0.0001). Importantly, they found a
clear relationship between hibernating myocardium and improvement
in left ventricular ejection fraction. There was a linear
trend between change in left ventricular ejection fraction
and number of myocardial segments with hibernation (p=0.009).
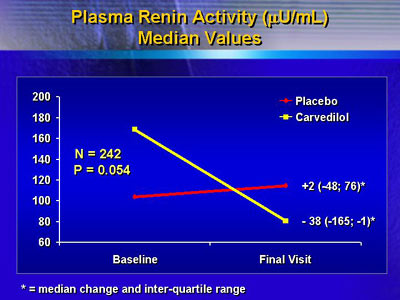
At the current meeting, Dr. Cleland reported on plasma renin
activity from 242 patients in CHRISTMAS. Plasma renin activity
tended to fall on carvedilol. The median change in plasma
renin activity was a decrease of 38µU/mL for carvedilol
vs. an increase of 2µU/mL for placebo. This trend approached
statistical significance (p=0.054).
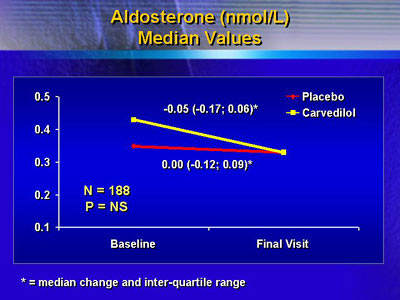
Investigators also had aldosterone concentration data for
188 patients. They found a trend toward reduced aldosterone
concentrations on carvedilol. Aldosterone levels fell in the
carvedilol group (median of 0.05 nmol/L), and remained unchanged
in the placebo group (median 0.0 nmol/L). The difference between
the carvedilol and placebo groups was not statistically significant.
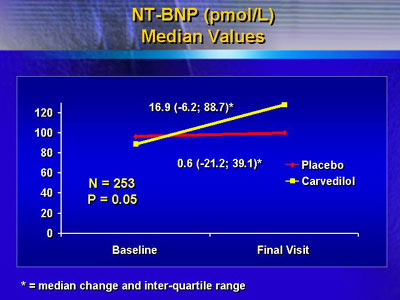
Finally, they noted an inverse relationship between the
fall in plasma renin activity and a rise in amino-terminal
pro-brain natriuretic peptide. Although levels were essentially
unchanged in the placebo group, they rose in the carvedilol
group.
These results may help explain why the combination of carvedilol
and an ACE inhibitor appears to offer a larger benefit than
either agent alone. The ACE inhibitor can cause very large
increases in renin, possibly weakening the effect of that
drug. Carvedilol, however, may then significantly reduce plasma
renin levels, and possibly further suppress aldosterone, as
investigators showed in this study.
|