The
CARMEN study provides an immediate mandate to prescribe the
combination of carvedilol and an ACE inhibitor in patients with
mild congestive heart failure (CHF), according to the investigator.
In addition, clinicians can now consider using carvedilol as
first line therapy in these patients.
Clinicians widely accept ACE inhibitors as
first line therapy for CHF. ACE inhibitors have become first
line therapy mainly because they were the first type of treatment
to be evaluated in clinical trials. However, carvedilol may
also be an acceptable first treatment for prevention of heart
failure progression and reversal of remodeling.
The objective of the CARMEN trial was to challenge
the prevailing practice of using ACE inhibitors as the mandatory
first choice in this setting. Investigators compared carvedilol,
enalapril and the combination of carvedilol and enalapril.
Treatment continued for 18 months.
This parallel-group randomized study included
479 patients from 13 European countries. All patients had
mild CHF, with left ventricular ejection fraction less than
40%. Most patients (65%) had NYHA Class II heart failure.
The mean age was 62 years, and 81% were men.
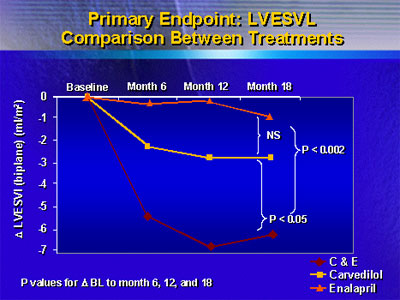
Investigators assessed effect on left ventricular
remodeling with transthoracic echocardiography at baseline,
then at 6, 12 and 18 months. The primary endpoint of the study
was change in this parameter from baseline to 18 months.
The following illustration shows that there
was a significant improvement in left ventricular remodeling
and function in the group of patients that received the combination
of carvedilol and enalapril:
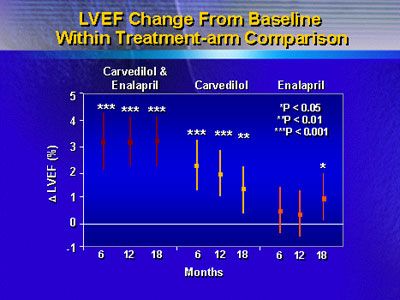
Furthermore, investigators observed reversal
of left ventricular remodeling in patients who received carvedilol
as monotherapy or in combination with enalapril. At 18 months,
they saw an increase in left ventricular ejection fraction
of approximately 3% in the combination group (p<0.001 versus
baseline). These results did not occur in the enalapril monotherapy
group.
Safety and tolerability was very similar in
all three treatment groups. Serious adverse events occurred
in 29% of patients in the carvedilol arm and in 28% of patients
who received carvedilol plus enalapril. Adverse events leading
to withdrawal occurred in 18% of patients in both groups.
Dr. Remme added that there was no difference in tolerability
between carvedilol and enalapril.
Dr. Remme said these results challenge the
standard practice of prescribing an ACE inhibitor, then later
prescribing a beta blocker if the patient remains symptomatic.
Currently, guidelines in both the United States and Europe
say that an ACE inhibitor should be first line treatment.
Dr. Remme helped draft the 1997 and 2001 guidelines of the
European Society of Cardiology. Now he thinks future guidelines
should no longer state that ACE inhibitors need to be the
first choice.
The results of this study give clinicians
sufficient reason to consider using carvedilol or this combination
as first line therapy, according to the investigator. Further
research may show that first line carvedilol may produce better
outcomes in certain patient populations.
|