| This
trial compared stenting plus directional coronary atherectomy to stenting
alone in complex lesions. Overall, stenting plus atherectomy was not
superior to stenting alone in improving angiographic binary restenosis.
However, investigators did not always achieve optimal directional
atherectomy. In addition, the combination approach may be better than
stenting alone in more complex lesions.
The study of techniques that may improve the effectiveness of stent
interventions continues to be an important area of research. One
potential approach is prior debulking of the lesion using directional
coronary atherectomy.
Investigators evaluated this approach in the Atherectomy before
Multi-Link Improves Lumen Gain and Clinical Outcomes (AMIGO) trial.
The purpose of AMIGO was to compare stenting with or without adjunctive
atherectomy in native coronary arteries (de novo or restenotic).
The primary endpoint was angiographic binary restenosis at 8 months.
The study included 753 patients randomized to stent plus directional
coronary atherectomy or stent alone. By study design, all patients
had complex lesions, including lesion length greater than 12 mm,
bifurcation, ostial lesions or total occlusions. About a third of
patients received abciximab (ReoPro). There were no important differences
in baseline characteristics between the two groups.
Stent plus atherectomy provided better immediate angiographic results.
However, at 8 weeks, the rate of binary restenosis was 19.6% in
the stent only group, and 24.1% in the stent plus atherectomy group
(P = 0.22). Yet the use of directional atherectomy did not increase
incidence of complications in the short term or at one year.
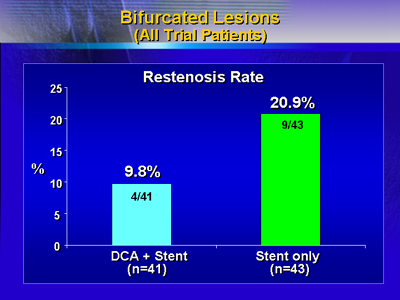
For bifurcated lesions only, the restenosis rate was 9.8% for the
combination approach, vs. 20.9% for stent only. Due to the small
sample size, the finding did not reach statistical significance.
These results cast doubt on the possibility that directional atherectomy
will improve lumen gain and outcome in the treatment of coronary
artery lesions.
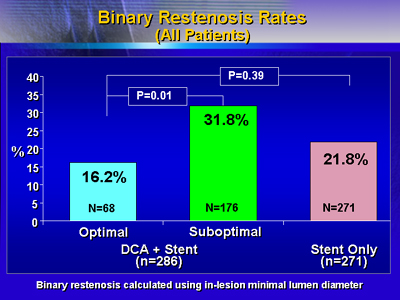
However, investigators achieved optimal directional atherectomy
in only 21.5% of cases. In fact, stent plus atherectomy appeared
superior to stent alone in centers that achieved an optimal result
more frequently. Binary restenosis rates were significantly lower
in patients who received optimal directional atherectomy vs. those
who did not.
In addition, the expected rate of binary restenosis in the stent
only group was 30%, as opposed to the actual 19.6% investigators
reported. This lower than expected restenosis rate suggests the
lesions treated may have been too favorable. Centers that treated
more complex lesions had better success with stenting plus atherectomy.
Because of these factors, Dr. Colombo and colleagues still perform
stenting plus directional coronary atherectomy in selected cases.
|
