| In
the final results of this study, patients who received stents with
thinner struts had significantly lower restenosis rates than patients
who received stents with thicker struts. The results suggest that
strut thickness and design have a significant impact on long-term
patient outcomes.
Previous research shows that different stents yield different outcomes.
One randomized comparison of 5 stents showed a striking variation
in angiographic restenosis rates (25% to 36%) and target vessel
revascularization rates (14% to 29%). These differences suggested
specific stent characteristics could affect the development of restenosis.
Subsequently, investigators compared two stents with similar design,
but different strut thickness in a trial named Intracoronary Stenting
and Angiographic Results-Strut Thickness Effect on Restenosis Outcome
(ISAR-STEREO).
One stent was a first generation Multi-LinkTM. It had
very thin struts (50 microns). The other, a second generation Multi-Link
Duet, had a strut thickness of 140 microns. At 6 months, there was
significantly less restenosis and target vessel revascularization
with the thinner strut stents.
The goal of ISAR-STEREO-2 was to assess restenosis and long-term
outcome in stents of different design. Investigators from four German
centers randomized 611 patients to receive the same thin strut Multi-Link
stent, or a thick strut stent of different design (Cordis BX Velocity).
The Multi-Link stent has characteristic interconnected rings, while
the Cordis stent has a closed cell, flexible segment design.
All patients had to have symptomatic coronary artery disease and
lesions in native coronary vessels no larger than 2.8 mm. The primary
endpoint was rate of angiographic restenosis at 6 months. There
were no significant differences between patient characteristics
or cardiovascular risk factors.
Significantly more patients in the thin strut stent group had ACC/AHA
classification B2 or C lesion types. On the other hand, there were
more chronic occlusions in the thick strut stent group.
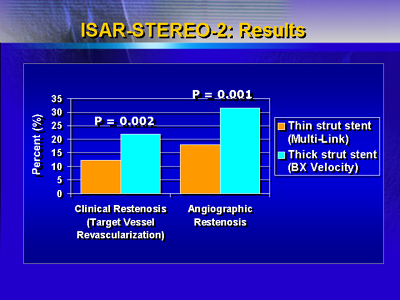
At 6 months, the rate of angiographic restenosis was 17.9% in the
thin strut stent group and 31.4% in the thick strut stent group
(P < 0.001), a 43% reduction.
A secondary endpoint was clinical restenosis at 6 months. The target
vessel revascularization rate was 12.3% for the thin strut stent
group and 20.9% for the thick strut stent group (P = 0.002), a 44%
reduction.
Another secondary endpoint was survival free of myocardial infarction
at 12 months, but there was no significant difference between the
thin strut group (95.1%) and the thick strut group (93.7%).
Experts once assumed that the most important factors in restenosis
were lesion characteristics, implant techniques and other nuances.
Now, ISAR-STEREO-2 suggests stent thickness and design may have
an enormous impact.
Cordis Germany partially funded this study.
|
